
Sinus lift
Sinus lift procedure
When performed by an expert, the sinus lift is one of the safest methods of bone reconstruction for the posterior area of the upper jaw! The so-called sinus lift procedure is commonly feared by patients. But unjustly so, in our opinion! Scientific documentation and our more than 20 years of successful experience with this procedure confirm this statement.
A sinus lift is necessary whenever the residual bone of the upper jaw is reduced in height, for example through expansion of the maxillary sinus. Today, it is assumed that an implant length of 11 mm (for a respective implant diameter > 4.1 mm) is required to ensure safe and long-term anchoring of implants. In many cases, this residual bone height is no longer available due to anatomical reasons or prior loss of tooth or bone material. The minimum height thus must be restored surgically, and the floor of the maxillary sinus lifted accordingly (“sinus lift”).
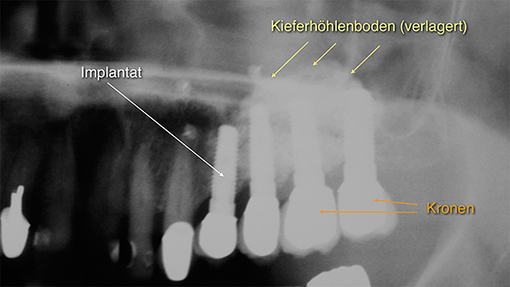
Figure 1: Patient case
Patient case with reduced bone height in the upper jaw (premolar/molar area); the residual bone height is insufficient for anchoring implants. The floor of the sinus must be raised surgically (sinus lift procedure).
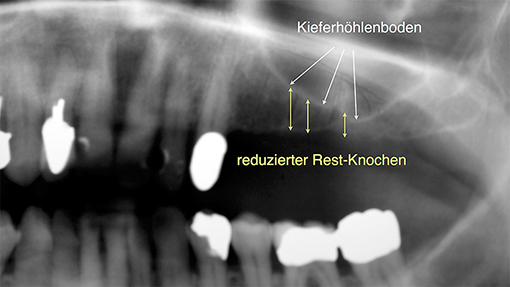
Figure 2: Patient case 2
X-ray image after 4 years of implant function: Lifting of floor of maxillary sinus (sinus lift), grafting of bone replacement material. Following the healing period, implants were placed and subsequently supplied with crowns.
As the x-ray image of the patient case shows, room for bone augmentation was created by lifting the floor of the maxillary sinus. Placement of the implants was not possible until bone grafting. The implants are placed in the newly-augmented bone and subsequently supplied with individual crowns.
Figure 2 shows a patient case following 4 years of implant function. This patient was able to do without partial dentures and opt for implants.
Surgical approaches
In general, two surgical methods are available: the closed surgical approach ( Summers 1994) and the open technique (Tatum 1986).
Minimally-invasive closed method
The closed method, also referred to as the minimally-invasive method, allows for lifting of the floor of the maxillary sinus via the drill hole of the implant with special elevators. This method should only be applied if sufficient residual bone height is present. The original surgical method (Summers 1994) and our own experience have shown that a safe lift of approx. 3 mm of the floor of the maxillary sinus is possible. Refined techniques and instruments continue to advance this method. In many cases, a comprehensive, open sinus lift can be avoided!
The following figure, obtained from the textbook “Checklist – Implantology” (Authors: Cacaci, Neugebauer, Schlegel, Seidel, Thieme Publisher) details the procedure.
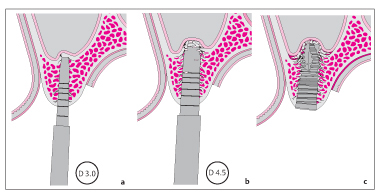
Figure 3
Schematic diagram of the approach from “Checklist – Implantology” (Cacaci et. al); after drilling for the implant to a depth of just before the floor of the maxillary sinus, the maxillary floor is slightly lifted using specialized instruments.
This method is regarded as “minimally-invasive” as the sinus lift is performed via the drill hole of the implant. Application of this method reduces additional side effects such as facial swelling and pain. However, the degree of bone height augmentation is limited.
Open method
The open, traditional surgical method was pioneered by the American dentist, Tatum, in 1984. It has been safely applied in our practice since 1993.
This surgical method is characterized by lateral access to the maxillary sinus from the oral vestibule. It rarely causes complications and is an outstanding method to perform vertical bone grafting in the premolar/molar area of the upper jaw. The following schematic, obtained from the textbook “Checklist – Implantology” (Authors: Cacaci, Neugebauer, Schlegel, Seidel, Thieme Publisher) details the procedure:
Figure 4
a: the mucosa is lifted from the residual jaw bone
b: laterally from the jaw, the maxillary sinus is gently opened without damaging the mucosa of the maxillary sinus
c: the mucosa of the maxillary sinus is gently loosened from the floor of the sinus, thereby creating room for the bone mass
d: in many cases, bone mass and implant can be placed simultaneously; the lateral access is closed again
Lifting the floor of the maxillary sinus creates an empty space that can be filled with bone material. Often, bone replacement materials mixed with the patient’s own blood can be used, eliminating the need for bone extraction from another part of the body. The healing time associated with this procedure is generally longer. But bone substitutes cannot always be used: scientific research has shown that in cases with a residual bone height of only 2 mm, only a graft from the patient’s own bone (obtained from the iliac crest or the lower jaw) presents a secure bone foundation for implants. In these situations, it is recommended that a bone graft from the patient’s iliac crest or low jaw is obtained. Which extraction site is more suitable depends on the individual patient.